The CD4 T-cell (also called T-cell, T-lymphocyte, or T-helper cell, or just plain CD4) is the white blood cell that HIV attacks, takes over, and eventually kills. If HIV is “enemy soldiers,” your CD4 count is your own army of individual soldiers. If you have close to 1000 of your own soldiers, that’s good. Two hundred or less of your own soldiers--not so good.
Remember back in high school biology class we learned that our body has 3 types of blood cells--red blood cells (erythrocytes) which deliver oxygen to our cells, white blood cells (also called leucocytes), which fight infection, and platelets (thrombocytes), which help the blood to clot? Well, lymphocytes, along with monocytes, basophils, neutrophils, and eosinophils are types of white blood cells.
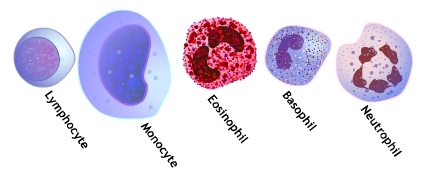
There are three types of lymphocytes--T-cells, B-cells, and natural killer cells. Just like brothers and sisters don’t look exactly look alike, you can tell the CD4 cells apart from the B-cells and natural killer cells by a tiny projection on the cells’ outer surface, called a T-cell receptor. The reason it’s called a T-cell is because these cells mature in the thymus gland, a gland that’s located in the center of the chest.

The CD4 count is the actual number of CD4 cells that can be found in one microliter of blood. To give you an idea of how small a drop of blood we are talking about, a microliter is one-millionth of a liter and a liter is around 4 cups. The drop is smaller than the head of a pin.
The CD4 T-cell count tells you when you should start HIV medicines and if it is okay to wait. If your CD4 count is normal--say 500-1500, you may want to wait before starting HIV medicines. If it is low, especially less than 200 or so, it is time to start HIV medicines.
The CD4 count also tells you when you need to take special antibiotics to prevent infections. In most cases, you will be given antibiotics to prevent certain infections when your CD4 goes down to 200 or so. If you are taking HIV medicines and your CD4 count goes up, and stays up--and your virus level is low--you can usually stop the antibiotics.
So, how exactly does HIV affect the CD4 T-cell count? Immediately after the virus enters the body, there is usually a sudden decrease in the CD4 count. Over the next several weeks, the CD4 will bounce back to nearly what it was before infection. For example, if you start with a CD4 around 1000, your CD4 may decline to around 500 in the month or two after infection, only to return to around 900-1000 at the three month point. In rare cases, the CD4 count may remain low. After this bounce-back, the CD4 will usually slowly decline over several years as HIV continues to destroy the CD4 cells.
On HIV medicines, the CD4 count will increase around 50 to 120 cells the first 3 months on medicines, then the increase slows down to an average of 2 to 7 cells a month. This slow rise can go on for years. The higher the person’s CD4 count when they start medicines, the more likely it is that they will achieve a “normal” CD4 count. If the virus is suppressed on the medicine, the CD4 will generally move upward. Some other factors, like illness, age, and unknown reasons, may cause the CD4 to remain low, even with no detectable HIV (undetectable viral load) in the blood.
A normal CD4 count is an adult is usually between 500 and 1500 with an average around 1000. You can see that this is a pretty wide range. The CD4 count varies by time of day, season, any new viral or bacterial infections you may have, and recent surgery. Steroids, vaccinations, chemotherapy, and hepatitis C medicines also affect the CD4 count. Removal of the spleen causes the CD4 to go up rather dramatically. In addition, factors like gender (male or female), pregnancy, race, age, and physical as well as psychological stress affect the CD4 count.
It is not unusual for patients who watch their CD4 counts closely to become quite upset when their CD4 counts decrease, or conversely, to be ecstatic by an increase in their CD4. While a CD4 decrease is concerning, the decrease must be put in the context of the total CD4 picture over time. One decrease (or even two) may just be the normal day to day variation of the CD4. It is much better to look at the entire trend of what the CD4 count is doing.
CD4s do not increase (once you are on medicine) or decrease in a straight line. Rather they will zig-zag upward or downward.
Month
|
0
|
1
|
2
|
4
|
6
|
9
|
CD4
|
100
|
150
|
200
|
175
|
205
|
232
|
CD4 percentage
|
9.0
|
11.0
|
12.5
|
13.1
|
13.8
|
15.0
|
You can see how the percentage number keeps slowly increasing but the actual CD4 count goes up and down. The percentage is very useful in telling us whether a CD4 count decrease is real.
Let’s look at 2 examples of how the CD4 percentage may give us more information than just looking at the CD4 count alone:
2 Examples of using the CD4 percentage to find out whether a decrease in CD4 count is real:
Example #1
Juan has been on HIV medicines for nearly one year. His CD4 count had increased from 3 to 333; however, at this visit, Juan’s provider tells him his CD4 has decreased to 255. Juan has no detectable HIV in his blood, and has not been missing any HIV medicine doses so Juan doesn’t understand why his CD4 has gone down. His provider shows him the numbers from the lab: when Juan’s CD4 was 333, his CD4 percentage was 21%; now that his CD4 count is 255, his CD4 percentage is 21.2%--in other words, nearly the same. This is good and shows Juan and his HIV specialist that the CD4 count decline is just temporary.
Example #2
Jane has also been on HIV medicines for nearly a year. Her CD4 count has risen from 7 (with a CD4 percentage of 2%) to 261 (CD4 percentage of 18%). Unlike Juan, Jane has had some issues with her new boyfriend and a new job and has been skipping her once a day HIV medicines around 2 times a week. At her latest office visit, her provider tells her that her CD4 is now 252--just a slight drop--and she remains with undetectable HIV in her blood. However, her provider tells her that her CD4 percentage has gone from 18% to 12%. Her provider is worried--although the CD4 count is not really changed and Jane remains with no detectable virus, the CD4 percentage drop and the fact that Jane is missing her HIV medicines gives her provider a clue of what is to come. If Jane continues on her same path of missing her HIV medicine, it will not be long before Jane’s CD4 will be headed downward and her virus becomes detectable.
As a general rule, the CD4 is checked every 3-4 months for the first few years on HIV treatment. Some HIV specialists may move this to every 6 months if the CD4 goes into the normal range (500-1500) and remains there for more than 2 years or so.
From: Guidelines for the Use of Antiretroviral Agents in HIV-1 Infected Adults and Adolescents, January 10, 2011
This comment has been removed by a blog administrator.
ReplyDelete